
Could a community centred take on medical schools help New Zealand’s GP shortage?
The growth of New Zealand’s population together with an ageing society with increasingly complex health and social care needs has placed a greater demand on statutory care services.
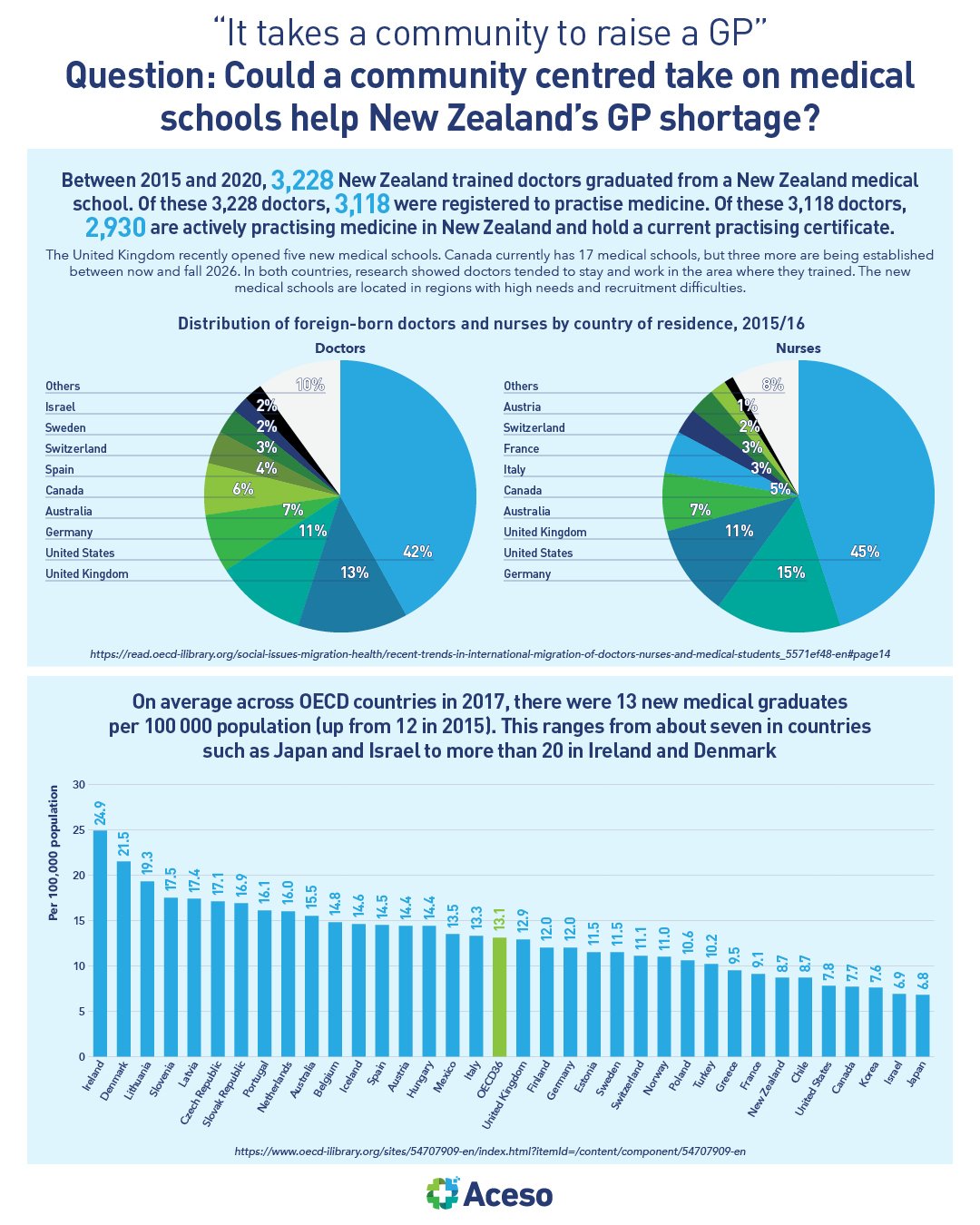
"It takes a community to raise a GP". Over the course of the past 60 years, we have seen a major shift in medical school education across much of the world, wherein it moved the teaching and training of new doctors from communities into universities, where they learned basic sciences; and hospitals, where they got hands-on experience in patient care and research. These big university-affiliated teaching hospitals are where students now spend much of their time, but most people get their healthcare through a family doctor or walk-in clinic, which sees a much wider range of problems. There is a school of thought that posits medical education returning to the community, purported to be a crucial piece in training and retaining more family and community doctors.
The Northern Ontario School of Medicine in Canada for example, pioneered an approach in which medical students learned their core clinical medicine in family practice clinics, community health centres, elder care facilities and community mental health services, seeing patients early in their training, in locations where it's hoped they will serve after they complete their degrees. They call it the 'cradle to grave approach', seeing students start their learning starting in their own community, to serving their own community, to retiring in their own community.
It is designed from the ground up on the principles of social accountability, equity, diversity and inclusion and reconciliation, an innovative approach to health education meant to address the growing gaps in primary care, especially in diverse and fast-growing regions. It will probably be another 10 years before the effects of such an approach are felt, but the proposal is meeting with pushback from the current workforce who are concerned they will be told to teach on top of maintaining their patient load, which they worry will lead to burnout for them, a poorer learning experience for students and a lower level of care for patients.
The example is a good real world scenario to keep a watchful brief on, as we navigate the challenges in our health sector, here in New Zealand.